2019-04-12
作者:广东省肺癌研究所 杨学宁 & LAMP
肺结节GGO内部和周围的影像组学特征可能区分微小浸润和原位癌
162. Radiomic CT Textural Features Inside and Adjacent to Ground Glass Lung Nodules Can Distinguish Minimally Invasive and Adenocarcinoma in Situ from Invasive Adenocarcinoma: A Multi-Site Study
*Philip A. Linden1, Pranjal Vaidya2, Kaustav Bera2, Robert Gilkeson1, *Christopher W. Towe1, Prabhakar Rajiah3, Frank Jacono4, Matthew J. Bott5, Adam J. Bograd5, *David R. Jones5, Kevin Li-chun Hsieh6, Gong-Yau Lan6, Anant Madabhushi1
1University Hospitals Cleveland Medical Center, Cleveland, OH;2Case Western Reserve University, Cleveland, OH;3University of Texas Southwestern Medical Center, Dallas, TX;4Cleveland VA Medical Center, Cleveland, OH;5Memorial Sloan Kettering Medical Center, New York, NY;6Taipei Medical University, Taipei, Taiwan
Invited Discussant: *Isabelle Opitz
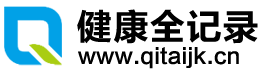
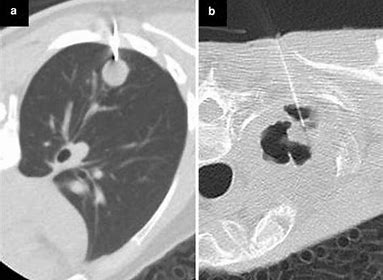
Objective: Lepidic cancers follow an orderly progression from adenocarcinoma in situ (AIS) to minimally invasive carcinoma (MIA) to invasive adenocarcinoma (INV). The presence of a nodular component on CT suggests an invasive component, but neither conventional CT nor needle biopsy can accurately determine invasive disease in early lepidic lesions. We sought to develop an imaging derived method to differentiate these clinical entities in order to guide treatment.
Methods: Preoperative CT scans and coexisting pathology reports of 93 invasive and 54 specimens with minimal or no invasion were collected from three medical centers. Only T1a INV were chosen (predominantly GGO <=2cm diameter), matching the diameter of the MIA subset (<=2cm). The first site (N=39) was used for training the classifier which contained 7 AIS and 2 MIA and 30 INV. In order to have a true independent validation cohort, patients from two sites were kept blinded to the model. The validation set included 108 patients, 63 INV and 45 MIA. A total of 248 radiomic texture features from inside the tumor (intratumoral) and immediately adjacent to the nodule (peritumoral) were extracted from within and outside the manually annotated lung nodule. The top five discriminative features were selected using a statistical feature selection algorithm, and a Linear Discriminant Analysis (LDA) machine learning classifier was trained in order to distinguish between the two classes.
Results: The top five selected stable features included 4 from inside the tumor (2 Haralick features, 1 Gabor, 1 Collage) and 1 from immediately outside the lung nodule (1 Collage) (0-3mm). The machine learning model successfully differentiated INV from MIA and AIS with an AUC of 0.97 (p<0.05) (sensitivity - 95.5%, specificity – 94%). Textural features from within the nodule reflecting on the tumor heterogeneity were found to be the most predictive followed by peritumoral features from 3mm outside the tumor region. Peritumoral analysis of 3mm rings outside the tumor, as far as 9mm from the edge of the tumor also showed AUC values of 0.930 in discriminating MIA from INV.
Conclusions: Radiomics assessment of routine chest CT scans provides a non-invasive way to determine the degree of invasion in lung adenocarcinomas, being able to distinguish between non/minimally invasive and invasive lung cancer. Such information is useful in determining need for, and timing of, resection. Prospective multi-institutional validation should be pursued.







推荐阅读
文章评论
注册或登后即可发表评论
登录/注册
全部评论(0)