2019-04-13
作者:广东省肺癌研究所 杨学宁 & LAMP
影像引导的电视辅助胸腔镜切除术
268. Image Guided Video Assisted Thoracoscopic Resection (iVATS): Translation to Clinical Practice
Ritu R. Gill1, Julliane Barlow2, *Michael T. Jaklistch2, Abraham Lebenthal2, *Yolonda L. Colson2, Christopher Ducko2, Eric Schmidlin2, Phillip M. Hartigan2, *Raphael Bueno2
1Beth Israel Deaconess Medical Center, Boston, MA;2Brigham & Women's Hospital, Boston, MA
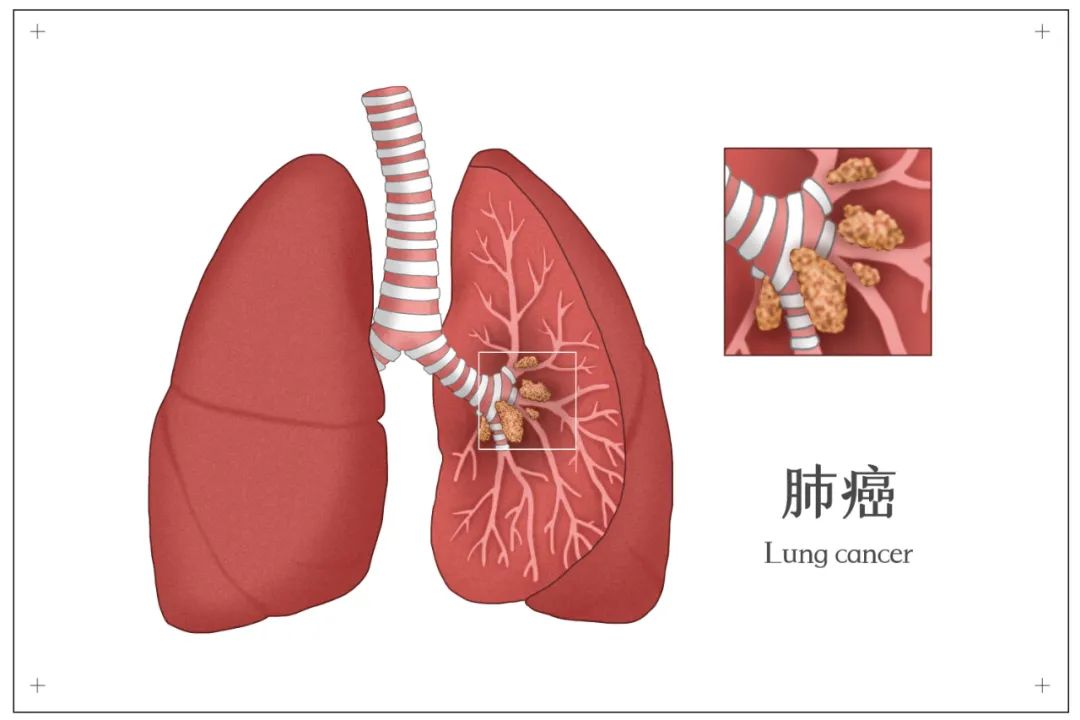
Objective: We developed a novel approach to facilitate localization and resection of sub- centimeter lung nodules, combining placement of fiducials using intraoperative Cone beam computed tomography (CT) guidance with standard thoracoscopic resection technique using image-guided video-assisted thoracoscopic surgery (iVATS) (J Surg Oncol. 2015). We report our experience of translating iVATS into clinical care.
Methods: Methodology and workflow for iVATS developed as part of the Phase I/II trial was used to train surgeons, radiologists, anesthesiologists and radiology technologists. Intra-operative Cone beam CT scan was utilized for guidance of percutaneous placement of two T-bars (Kimberly-Clark, Roswell, GA) to localize the nodule followed by VATS resection of the tumor in the research operating room. Patients deemed suitable for the approach were consented by their surgeon. Radiation dose, time from induction to incision, placement of T-bar to incision and incision to closure, hospital stay and complication rates were recorded.
Results: Between 2015 and 2018, 42 patients underwent iVATS for the resection of 46 nodules in a clinical hybrid OR. Nodule size ranged from 0.6-2.5 cm (mean = 1.3 ± 0.38 cm). Forty-five nodules (97%) were successfully resected, 1(2%) had a positive margin and 1 (2%) could not be resected, as patient was unable to tolerate single lung ventilation. Ten (22%) were solid, 7(15%) had >50% ground-glass component, 10(22%) had >75% ground-glass component, 3(7%) nodules were 100% ground-glass. Distance of nodule from the pleura was 0-3.8 cm. Thirty-six (78%) were adenocarcinomas (3(7%) adenocarcinoma in situ, 2(4%) minimally invasive adenocarcinomas with an invasive component of 0.1 cm), 1(2%) squamous cell carcinoma, 4(9%) metastases and 4(9%) benign diagnosis (2(4%) organizing pneumonia, 1(2% pneumonia, and 1(2%) lymphocytic interstitial pneumonia. Stage groupings for the lung cancers (8th edition)-5(11%)TiasN0M0, 11(24%)T1aN0M0, 10(22%)T1bN0M0, 7(15%)T1cN0M0 and 1(2%) T2aN0M0. Thirty-seven (80%) patients underwent wedge resection, 4(9%) lobectomies and 1(2%) segmentectomy. Four (9%) patients had 2 lesions resected during the same procedure. Average and total procedure radiation dose was in the acceptable low range (median = 1572 μGy*m2, range 229-4372). Time from induction to incision was 81 minutes median; (Range13-157 minutes). Time from placement of T-bar to incision median 12 minutes (4 - 55 minutes); incision to closure 120 minutes (41-212) minutes. There were no deaths, and all patients were discharged from the hospital (median length of stay = 3 days, range 1-12).
Conclusions: Translation of iVATS into clinical practice has been initiated using a safe step-wise process, combining intra-operative C arm CT scanning and thoracoscopic surgery in a hybrid operating room.







推荐阅读
文章评论
注册或登后即可发表评论
登录/注册
全部评论(0)